












Young Adults With Type 2 Diabetes: A Journey Begins: Taking the Long View
Cardiology
Medscape
News & Perspective
Your one-stop resource for medical news, clinical reference, and education.
Sign up for FREEAlready a member? Log in
UK News & Perspectives View All
Featured Cardiology News & Perspectives
Latest News View All
-
Too Little CV Risk Factor Control Seen in Patients With APS
-
 Does Mental Illness Affect Emergency Response to Chest Pain?
Does Mental Illness Affect Emergency Response to Chest Pain? -
 Consider Chronic Pain When Screening for Hypertension
Consider Chronic Pain When Screening for Hypertension -
 Why Doctors Relocate Globally — And What LATAM Reveals
Why Doctors Relocate Globally — And What LATAM Reveals -
 What Foreign Doctors Need to Know About Working in Spain
What Foreign Doctors Need to Know About Working in Spain -
 Germany: A Magnet for Foreign Doctors, but Losing Its Own
Germany: A Magnet for Foreign Doctors, but Losing Its Own -
 The World’s Doctors Are on the Move — Italy Is Hit Hardest
The World’s Doctors Are on the Move — Italy Is Hit Hardest -
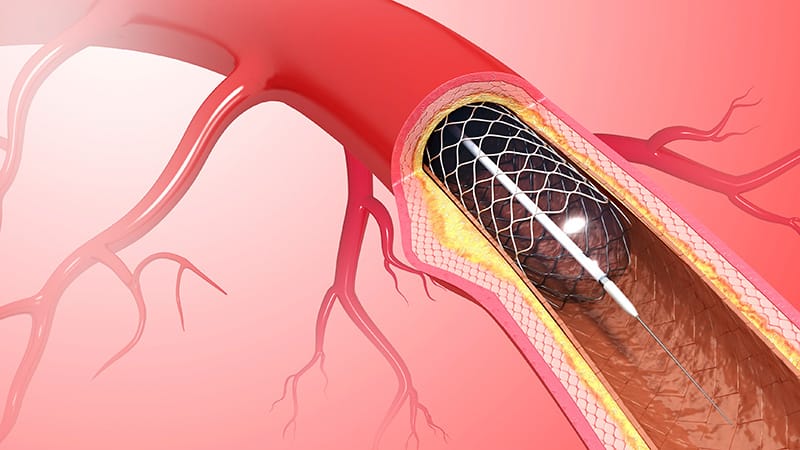 A Two-Step PCI for Blocked Arteries: Does Timing Matter?
A Two-Step PCI for Blocked Arteries: Does Timing Matter?
Trending With Cardiologists
Perspectives View All
Columnists
mtv




Journal Articles View All
-
Nonsteroidal and Steroidal Mineralocorticoid Antagonists
-
Binary Thresholds for Hypercholesterolemia and Hypertension
-
Dietary and Lifestyle Habits of Cardiologists
-
Expanded Definition of Worsening HF: Impact on Outcomes and QoL
-
Switching OAC and Managing Complexity in Frail Patients With AF
-
Aldosterone Modulation in Cardio-Kidney Diseases
Medscape Essentials


Cases & Quizzes View All

Conferences View All
View AllBusiness of Medicine View All


Medscape Editorial Collaborations
Advisory Board
EXECUTIVE EDITORS
Chief Cardiology Correspondent


